Article Text

Abstract
Objective Electronic nicotine delivery systems (ENDS), such as e-cigarettes, have surged in popularity. While long-term risks remain unclear, known dangers include nicotine addiction, E-cigarette or Vaping Use-Associated Lung Injury and potential extrapulmonary effects on the heart, immune system and neurodevelopment. Addressing ENDS addiction may require strategies akin to smoking cessation. However, evidence is lacking; there are no currently approved vaping-cessation aids. The objective of this review is to summarise the available literature addressing interventions for vaping cessation.
Data sources and study selection A librarian-assisted search was conducted in MEDLINE, Embase and Scopus, as well as preprints in Europe PMC, Open Science Framework, and the grey literature searches until January 2024. Six included studies used self-report methods to determine the abstinence rate, while one study used cotinine-level-verified self-reported abstinence. We included randomised controlled trials (RCTs) that examine ‘rates of vaping cessation’ outcomes. An intention-to-treat approach was used for data extraction, and random-effects meta-analyses models were applied.
Data synthesis Seven RCTs were included, which studied pharmacological therapy, digital interventions and/or educational content. The primary meta-analyses demonstrated a statistically significant increase in the odds of achieving 7-day point prevalence abstinence (PPA) (OR 1.52, 95% CI 1.15 to 2.01, number of participants=3244, moderate-certainty) and continuous abstinence (OR 2.71, 95% CI 1.31 to 5.61, number of participants=164, low-certainty) following intervention. A non-significant increase in odds was noted at 30-day PPA (OR 1.32, 95% CI 0.72 to 2.42, number of participants=1994, very low certainty).
Conclusions Vaping cessation interventions increase 7-day PPA rates at 1–12 months follow-up and this was consistent across prespecified subgroup analyses of the intervention type, outcome and duration of follow-up. More high-quality studies with reproducible findings are needed to enhance the certainty of the evidence and guide clinical interventions.
PROSPERO registration number CRD42022383670.
- Cessation
- Electronic nicotine delivery devices
- Nicotine
- Vaping cessation
Data availability statement
Relevant data are included in the article or uploaded as supplementary information. Specific requests for additional data will be made available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
The prevalence of electronic nicotine delivery systems (ENDS) usage, particularly among youth and young adults, has risen significantly in recent years. While some literature supports the use of ENDS for smoking cessation, there are important public health concerns related to addiction, cardiorespiratory effects and limited long-term safety data. E-cigarette users are interested in quitting but have limited success, likely due to the lack of evidence-based interventions to help them quit.
WHAT THIS STUDY ADDS
This systematic review and meta-analysis provides critical insights into the effectiveness of interventions for vaping cessation by type of intervention and duration of follow-up. Our findings demonstrate a significant increase in the odds of achieving short-term vaping abstinence and continuous abstinence rates, particularly with pharmacological and educational interventions. This study fills a gap in understanding by quantifying the impact of various cessation strategies on ENDS users.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
The findings serve as the first meta-analysis of this topic, which will immediately guide clinical practice. At the same time, it highlights gaps in the literature to direct future research on evidence-based approaches for vaping cessation. This is important given the rise in recreational ENDS use, particularly among youth and young adults. Policy-makers can leverage these results to support the development of regulations and public health initiatives aimed at curbing ENDS usage.
Background
The use of electronic nicotine delivery systems (ENDS), such as e-cigarettes and vapes, has grown substantially in the past decade.1 Globally, approximately 15% of individuals aged 15 years and older have experimented with vaping products, with the highest rates observed among youth (15–19 years) and young adults (20–24 years).2 In the USA, rates of youth vaping reached as high as 23.9% (ever users) and 12.8% (current users) among those aged 18–20 years.3 4 Even in Canada, one in seven young Canadians reported vaping on a regular basis in 2020.5 6 Children and teenagers are at high risk of developing nicotine addiction from vaping, highlighting an urgent need to address this issue.7 8 Some formulations of ENDS have been noted to deliver very high levels of nicotine—far greater than is possible with conventional cigarettes.9 To curb this, Health Canada released regulations to lower the maximum nicotine concentration per device, from 66 mg/mL to 20 mg/mL in 2021 and to restrict e-cigarette flavours.10
Among e-cigarette users, the reasons for vaping vary from leisure to cigarette smoking cessation.11 There is growing literature describing the use of e-cigarettes to help reduce or quit smoking.12–15 However, there is evidence that when used serendipitously by people who smoke in the hope of achieving cessation, significant success is not forthcoming and that ‘dual use’ may occur commonly—with diminished likelihood of cessation success.16 In addition to such concerns, given the lack of long-term safety data, e-cigarettes are not considered first-line cessation aids.17 Recently, concerns have emerged regarding the cardiorespiratory consequences of inhaling heated vapours containing nicotine, flavouring and multiple other compounds.18 19
Before the COVID-19 pandemic, e-cigarettes represented a growing cause of acute lung injury termed E-cigarette or Vaping Associated Lung Injury (EVALI).20 A study from 2020 in the New England Journal of Medicine reported 2558 hospitalised non-fatal cases and 60 fatal cases of EVALI in primarily healthy individuals.21 Since this time, it has been shown that co-use of tobacco and e-cigarettes resulted in a fivefold increase in the likelihood of being diagnosed with COVID-19.22 Those who vape also experienced a higher frequency of COVID-19 symptoms when compared with age-matched and gender-matched individuals who do not vape.22
Research has explored whether individuals who vape are interested in receiving support for vaping cessation. One study reported that the majority (73.4%) had no intention of quitting vaping use.23 Multiple participants noted that they did not see a reason to quit, as vaping was considered a useful tool for quitting cigarettes. Subjectively, they felt that vaping was less deleterious than smoking.24 However, studies among adolescents have noted that a significant proportion of those who vape are ‘seriously thinking about quitting’ (45%) or ‘have tried to quit vaping completely’ (25%).25 Disturbing rates of vaping behaviours among youth (many of whom would not be likely to become smokers) and the rapid development of nicotine addiction in this population underscore the importance of establishing evidence-based approaches to vaping cessation.
While there is strong evidence supporting interventions such as counselling and follow-up, nicotine replacement therapy (NRT), varenicline, cytisine and bupropion in facilitating cigarette smoking cessation, less is known about the approaches that may facilitate the cessation of vaping.26 27 There exists no widely accepted standard of care for vaping cessation. Nonetheless, this remains an important challenge facing clinicians. In the absence of high-quality evidence and guidelines, some practitioners have attempted to use established smoking cessation strategies ‘off-label’ for vaping cessation with unclear effect. The aim of this systematic review and meta-analysis is to summarise and synthesise the results from RCTs of interventions aimed at vaping cessation. This will guide clinical practice and the development of future guidelines while identifying gaps in knowledge and stimulating future research.
Methods
This systematic review and meta-analysis is reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2020 Guidelines.28 The protocol study for the current systematic review and meta-analysis was preregistered with PROSPERO (CRD42022383670)
Data sources and searches
A librarian designed and peer-reviewed search strategy was conducted on 9 May 2022, and most recently updated on 17 January 2024, in MEDLINE, Embase and Scopus (see online supplemental file 1).29 No limits to language or publication date were applied; however, conference abstracts were eliminated from Embase results prior to export. A search for preprints was conducted in Europe PMC and Open Science Framework, and preprint results were limited by publication date to 2016–Present. Numerous websites identified via Grey Matters were handsearched.30 The main search concepts consisted of terms related to ENDS and cessation and were informed by previously conducted systematic searches.31–34 Search results were exported to Covidence (Melbourne, Australia) and duplicates were eliminated using the platform’s duplicate identification feature.
Supplemental material
Eligibility criteria
Studies were included irrespective of publication status, date of publication, risk of bias (ROB) or language. We included randomised clinical trials (RCTs). We excluded non-randomised prospective cohort studies, before-and-after (pre–post) observational studies, case series, case–control studies, cross-sectional studies and secondary sources (including review articles). We included studies of people who currently vaped (regardless of use of other substances including cigarette smoking) (Current users include daily vapers and non-daily vapers (occasional vapers) who have vaped within the past 30 days). We included studies that aimed interventions at the individual level (education, digital tools and pharmacotherapy). Studies that evaluated system-level interventions such as modification of e-cigarette flavours (eg, flavour ban, comparison of flavours) were excluded. Studies that examined individual abstinence endpoints were included. The definitions of abstinence in the included studies encompass both self-reported and biochemically validated measures. In this context, abstinence specifically refers to abstinence from vaping. Studies reporting changes in vaping rates at a regional level after a change in laws surrounding vaping were excluded. Studies not including these prespecified outcomes were excluded (including studies of ‘vaping sales’, ‘intention to try vaping’ and ‘online searches for vaping’). The reference list of included studies and related review articles was manually searched to identify other potential studies.
Study selection & data extraction
Each title and abstract were screened for eligibility independently by two reviewers (ALP, JB, MF, MS and JH). Full texts of the potentially eligible studies were retrieved. Reviewers then independently screened full texts in duplicate and recorded the primary reason for exclusion. Disagreements were resolved by a third reviewer (HM). Two reviewers (JH and ALP) independently abstracted data on intervention and outcome and recorded study and participant characteristics including age, sex, concurrent use, smoking status or use of other substances, previous quit attempts, study design, outcomes and study results. Review authors searched appendices and supplements of published articles. There was a 95% agreement rate between reviewers, and disagreements were resolved through discussion with a third reviewer.
Data synthesis
For studies with abstinence outcomes, point prevalence and continuous rates of abstinence were extracted. Point prevalence of abstinence was categorised and subgrouped (prespecified) by duration of abstinence follow-up (1–3 months, 4–6 months, 7–9 months or 10–12 months). In studies that measured outcomes across various time points, within-study analyses were performed to assess the impact of duration of follow-up on abstinence rates. Additional prespecified subgroup analysis was performed based on the type of intervention (digital, pharmacological and education). The statistical software STATA V.17.0 (StataCorp) was used to perform meta-analysis. ORs were computed by DerSimonian and Laird random effects models.35 Heterogeneity was assessed by Cochrane’s Q test (p value), which examines the null hypothesis that all studies are evaluating the same effect, and by Higgins’ test (I2), which quantifies inconsistency across studies and describes the percentage of the variability in effect estimates that is due to heterogeneity.36
Assessment of ROB
In duplicate, two review authors assessed ROB and an overall ROB score was assigned. For RCTs, reviewers evaluated the following domains from the Cochrane RoB 2.0 score: adequate randomisation sequence generation, allocation concealment, blinding of healthcare providers, blinding of participants, blinding of outcome assessors, blinding of statisticians, incomplete outcome data, selective outcome reporting and major baseline imbalance. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) Pro tool was used for the evaluation of the certainty of evidence regarding the outcomes.37
Results
Study inclusion
Figure 1 illustrates the flow diagram of the inclusion process and excluded studies. The final search resulted in 9399 papers, of which 5089 were removed as duplicates. A further 4222 papers were excluded after the title and abstract screen. 88 full texts were screened, of which 81 were excluded. Finally, seven RCTs38–44 were included in this systematic review and meta-analysis.

Flow diagram of study selection. RCT, randomised controlled trial.
Study outcomes
Table 1 summarises the main characteristics of the included studies. A total of 7 randomised clinical trials involving 5763 participants were included. All studies included were published after 2021. Six studies were conducted in the USA and one study was conducted in Italy. The sample sizes of the studies ranged from 30 to 2896 participants. Among these, five studies were conducted on exclusive e-cigarette users, while two studies included dual users (e-cigarette and conventional cigarettes). All included studies encompassed both males and females; proportions ranged from 33.3% to 63.0% males. The mean age of participants ranged from 20.3 to 52.6 years. Among the interventions, three studies used digital interventions (eg, smartphone applications, text messaging) either alone or in combination with other methods to enhance vaping cessation. Another three studies employed medical therapy (eg, NRT or varenicline) and counselling programmes, while one study solely relied on educational methods (ie, informational booklets). Follow-up evaluations of the participants ranged from 1 to 18 months. Five studies reported 7-day point prevalence abstinence (PPA), two studies reported 30-day PPA and two studies reported continuous abstinence rate (CAR) as an outcome. All included studies exclusively evaluated users of nicotine-containing e-cigarettes. Six included studies used self-report methods to determine the abstinence rate, while one study used cotinine-level-verified self-reported abstinence.
Study characteristics of included studies
Meta-analysis
Data from the seven RCTs were pooled to assess the impact of different interventions on vaping cessation.
Seven-day PPA
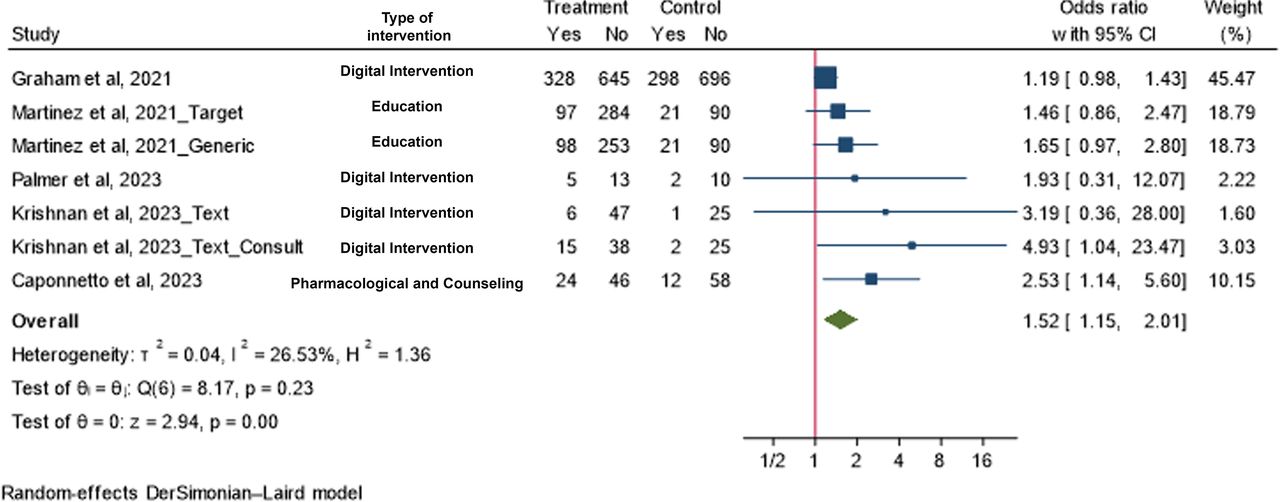
Four studies with six intervention arms comprising 3250 participants (1899 in the intervention group and 1351 in the control group) that reported 7-day PPA were meta-analysed. When pooled, the vaping cessation interventions were associated with 52% greater odds of achieving 7-day PPA compared with control (OR 1.52, 95% CI 1.15 to 2.01) (figure 2). Subgroup analysis based on length of follow-up indicated that the odds of vaping cessation were highest at 1–3 months follow-up (OR 3.29, 95% CI 1.16 to 9.35) and appears to reduce over time. Nonetheless, the odds of vaping cessation remained statistically significant at the 4–6 months (OR 2.53, 95% CI 1.14 to 5.60) and 10–12 months follow-up (OR 1.55, 95% CI 1.07 to 2.25). Visual assessment of the odds of vaping cessation over time on within-study subgroup analysis confirmed this decline in cessation rates of time (online supplemental file 2). Subgroup analysis also indicated that pharmacological interventions (OR 2.42, 95% CI 1.17 to 5.02) and educational interventions (OR 1.55, 95% CI 1.07 to 2.25) significantly increase the odds of achieving 7-day PPA. Digital interventions trended to increase the odds of achieving 7-day PPA, but this was not statistically significant (OR 1.95, 95% CI 0.73 to 5.22) (online supplemental file 2).
Supplemental material

Forest plot and meta-analysis of effect of vaping cessation interventions on 7-day point prevalence of abstinence.
Thirty-day PPA
Two studies with two intervention arms comprising 1994 participants (995 in the intervention group and 999 in the control group) that reported 30-day PPA were meta-analysed. When pooled, there was a trend to increase the odds of achieving 30-day PPA, but this was not statistically significant (OR 1.32, 95% CI 0.72 to 2.42) (figure 3).

Forest plot and meta-analysis of effect of vaping cessation interventions on 30-day point prevalence of abstinence.
Continuous abstinence
Two studies with three intervention arms comprising 164 participants (85 in the intervention group and 79 in the control group) that measured continuous abstinence at two and 6 months, respectively, were meta-analysed. When pooled, vaping cessation interventions were associated with a 2.7-fold statistically significant increase in continuous abstinence compared with control (OR 2.71, 95% CI 1.31 to 5.61) (figure 4).

Forest plot and meta-analysis of the effect of vaping cessation interventions on continuous abstinence rate. NRT, nicotine replacement therapy.
Quality review and certainty of evidence
The results of RoB 2.0 assessment found that four of the seven included RCTs were considered to have a low ROB, while the remaining three RCTs raise some concerns regarding biases (figure 5). The GRADE approach to assessing the certainty of evidence reveals that there is a low level of certainty for the ‘7-day PPA’ outcome. However, there is a very low level of certainty for the ‘30-day PPA’ and ‘CAR’ outcomes. See online supplemental file 3 for a detailed breakdown estimating the certainty of evidence.
Supplemental material

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Risk of bias assessment of included studies.
Discussion
We conducted a systematic review and meta-analysis of interventions aimed at vaping cessation. A total of seven RCTs of e-cigarette cessation interventions with abstinence were included. Multiple interventions were tested including educational content, digital tools and pharmacological interventions. The current meta-analysis found that vaping cessation interventions were associated with a 52% increase in the odds of achieving 7-day PPA and 2.7 times greater odds of CAR. Prespecified subgroup analysis confirmed a statistically significant, sustained 7-day point prevalence abstinence (PPA) over time, with a 55% increase in odds at the 10–12 months follow-up (OR 1.55, 95% CI 1.15 to 2.01) and by type of intervention. Specifically, a 2.42-fold increase in odds was observed with pharmacological interventions (OR 2.42, 95% CI 1.17 to 5.02), and a 55% increase with educational interventions (OR 1.55, 95% CI 1.07 to 2.25) compared with control.
This review has several strengths. To our knowledge, this is the first meta-analysis quantitatively assessing the effectiveness of vaping cessation interventions. This review provides a methodologically rigorous, quantitative and up-to-date summary of the literature. The search was updated as of January 2024 and incorporates both published and unpublished grey literature. The results are supported with a validated and thorough evaluation of the ROB and certainty of evidence. Subgroup analyses were performed to confirm consistency and effect over time and by intervention type. Both 7-day and continuous abstinence have been demonstrated as valid measures for assessing smoking and vaping abstinence in individuals who have quit.45
Recent reviews of ENDS use and their impacts have been published seeking to answer different research questions. A previous scoping review46 lacked adequate data to meta-analyse results to report a quantitative outcome and thus did not reach concrete conclusion about the effectiveness of vaping cessation interventions. A qualitative systematic review published in Cancer Prevention Research summarised the evidence on vaping cessation containing 79 studies, which included cross-sectional studies and case reports).47 It provided a summary of cross-sectional and qualitative studies examining the reasons for vaping cessation and e-cigarette user experiences (both of which were excluded from our review). Other systematic reviews have focused on e-cigarette use in pregnancy,48 vaping-related lung injuries,49 vaping and mental health comorbidity,50 and patterns of use for adolescent vaping.51 The lack of sufficient strong evidence meant that none of these reviews were able to make definitive conclusions about the impact of vaping on health or interventions that could help people quit.
There are several important limitations to consider in this review. First, there is a heterogeneity due to a few factors including the sample size, age, gender, exclusive or dual user, and intervention type (education, digital health or pharmacological). Furthermore, the included studies do not report relapse to smoking following vaping cessation interventions, which would be important to measure in future studies. The total number of studies is small with variability in the overlapping of the outcome type (1-day, 7-day, 30-day, continuous abstinence) and duration (ranging from 1-month to 18-month follow-up). This restricts our ability to leverage all the data for meta-analysis and to be able to perform more specific subgroup analyses. Nonetheless, subgroup analysis based on duration of follow-up showed a sustained 7-day PPA over time (including the longest follow-up duration of 10–12 months) with low heterogeneity. Subgroup analyses were not possible for the 30-day PPA and CAR outcomes over time given insufficient data but would be hypothesised to be similar to the findings of the 7-day PPA. Another important limitation of the included studies is that they measured abstinence at the end of treatment with limited long-term follow-up post-treatment, when relapse is more common. Consequently, it is unclear and unknown if the observed effects are sustained beyond the treatment period, highlighting the need for longer follow-up durations to assess long-term abstinence and relapse rates. Almost all participants included in the studies were adults limiting subgroup analysis by age. However, given the high prevalence of vaping among youth, future studies should focus on recruiting younger patients to test the efficacy of these interventions among this key group. In cases with significant variability in sample size, effect size in meta-analyses of RCTs can be driven by the results of the larger trials.39 Further, the quality of studies varied, driven by methodological differences and widely varying sample sizes. Among poor-quality studies, the primary issues of concern included low sample size RCTs and inability to blind participants. While Caponnetto et al used salivary cotinine testing for objective biochemical verification of vaping status, other studies used subjective self-report as the outcome measure, which can introduce bias and affect accuracy. Future studies should also use biochemical verification to improve rigour and study design. Given these limitations, the findings of the meta-analysis must be interpreted with caution. Nonetheless, we conducted a thorough review of the ROB and certainty of evidence. While the 30-day and CAR were very low and low certainty, respectively, there was moderate certainty for the 7-day point prevalence outcome. We also conducted analyses by type of outcome (7-day, 30-day or continuous abstinence), follow-up duration (1–3 months, 4–6 month, 7–9 months or 10–12 months), and intervention type (digital, pharmacological or educational). The point estimates for all studies favoured the intervention and the pooled estimates for all the primary and subgroup analyses trended towards favouring the intervention, either statistically significantly or non-significantly. These findings are encouraging for the use of an intervention to support vaping cessation, especially those that are educational and pharmacological. They may enable shared decision-making with patients for the use of interventions to quit e-cigarette use.
It is noteworthy to mention that some intervention methods may not be universally available worldwide. For instance, the specific digital interventions evaluated are only available in the USA.52 Pharmacotherapy, such as NRT and varenicline, is not approved for use in vaping cessation in most jurisdictions and thus must be used off-label. This also limits their routine use in RCTs without an arduous approval process. There have been ENDS-related regulatory interventions (eg, price, access and desirability (limits to flavours and marketing)) that have proven effective in reducing vaping but findings are insufficient to provide specific recommendations.53
There is a need for more well-designed RCTs leveraging diverse interventions for vaping cessation to improve the quality and certainty of estimates. However, the current review also highlights an important need to measure standard and consistent reporting of outcomes (7-day, 30-day and continuous abstinence) at multiple time points of follow-up within the same study to maximise the utility of the data for future meta-analyses.54 In addition, RCTs should aim to evaluate accessible and easily reproducible methods for vaping cessation including but not limited to text messaging, counselling, mobile applications, exercise, nutrition and pharmacotherapy. Given the behavioural differences and levels of dependency between conventional cigarettes and certain new, popular ENDS devices, coupled with the higher prevalence among younger demographics, it may be necessary to explore new and innovative interventions and combinations of strategies. Unique approaches may also be necessary to support exclusive e-cigarette users compared with those who also concurrently use tobacco. It is also critical to measure the impact of vaping cessation and associated interventions on the risk of switching or relapsing to conventional tobacco cigarettes. The studies in this systematic review did not report this outcome, which has important implications for harm reduction. On review of ClinicalTrials.gov, there are several RCTs underway evaluating vaping cessation, and we intend to update this systematic review and meta-analysis to identify gaps, encourage primary studies and to report the most up-to-date findings that can be applied in clinical practice.
Conclusions
Vaping cessation interventions increase 7-day PPA based on moderate certainty evidence and CAR based on low-quality evidence. This was consistent across prespecified subgroup analyses of the intervention type, outcome and duration of follow-up. However, there is an immediate need for more high-quality studies with reproducible findings. Future research should focus on implementing consistent and reproduceable vaping cessation interventions using high-quality study design through large RCTs and measuring diverse abstinence outcomes over multiple time points, especially post-treatment. This will provide much-needed guidance for patients, clinicians, researchers, administrators and policy-makers to support individuals to quit vaping.
Data availability statement
Relevant data are included in the article or uploaded as supplementary information. Specific requests for additional data will be made available upon request.
Ethics statements
Patient consent for publication
Acknowledgments
We thank Valentina Ly, MLIS (Health Sciences Library, University of Ottawa) for peer review of the MEDLINE search strategy.
References
Footnotes
JH and AP are joint first authors.
X @Javad_Heshmati_, @AvinashPandeyMD, @SVisin, @MullenKerri, @GuyattGH, @DrAndrewPipe, @drhassanmir
Contributors HM contributed to the conception, supervision and design of the research; SV contributed to the design of the search strategy and syntaxes; ALP, JB, MF and MS contributed to the screening and extraction of the data; GG and JH acquisition and analysis of the data; GG, K-AM and ALP contributed to the interpretation of the data; JH carried out the statistical analysis and HM, JH and K-AM drafted the manuscript. All authors critically revised the manuscript, agreed to be fully accountable for ensuring the integrity and accuracy of the work, and read and approved the final manuscript. HM is the guarantor and accepts full responsibility for the work and conduct of the study, had access to the data, and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests No, there are no competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.