Article Text

Abstract
Background Heated tobacco products (HTPs) are often marketed as a safer alternative to help cigarette smokers quit. We investigated the link between HTP use and smoking cessation and relapse.
Methods 7044 adults (≥20 years old) with at least two observations over three waves (2019–2021) of a longitudinal, nationwide, internet-based survey were classified into current (past 30-day), former and never cigarette smokers. ≥1 month and ≥6 months smoking cessation and smoking relapse at 1-year follow-up were assessed in relation to current HTP use at baseline. Generalised estimating equation models were weighted to account for population differences between HTP users and non-users. Adjusted prevalence ratios (APRs) were computed within population subgroups.
Results At baseline, 17.2%, 9.1% and 6.1% of the respondents were current cigarette smokers, HTP users and dual users, respectively. Among current established smokers (having smoked regularly, n=1910), HTP use was significantly associated with a decreased likelihood of ≥1 month cessation within those who reported having used evidence-based cessation measures (APR=0.61), smoking 20+ cigarettes per day (APR=0.62), high school education or less (APR=0.73) and fair/poor health (APR=0.59). Negative associations were also seen for ≥6 months cessation among those aged 20–29 years (APR=0.56) and full-time workers (APR=0.56). Among former smokers (n=2906), HTP use was associated with smoking relapse within those who last smoked >1 year ago (APR=1.54), among women (APR=1.61), those aged 20–29 years (APR=2.09), those reporting high school education or less (APR=2.36), those who were unemployed/retired (AOR=3.31) and never/non-current alcohol users (APR=2.10).
Conclusion HTP use did not help smokers quit or prevent former smokers from relapsing. HTPs should not be recommended as a cessation aid.
- Cessation
- Denormalization
- Non-cigarette tobacco products
- Surveillance and monitoring
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the author (TT) upon reasonable request.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Heated tobacco products (HTPs) are commonly used by cigarette smokers who attempt to quit smoking despite there being no evidence to support the utility of HTPs as a cessation aid.
WHAT THIS STUDY ADDS
HTP use was associated with decreased smoking cessation among established cigarette smokers who had used evidence-based cessation measures (counselling services/prescribed medications/over-the-counter nicotine replacement therapy products), those with a heavy smoking habit, with less education, with full-time work, with poorer health and among younger smokers.
HTP use also led former cigarette smokers to relapse to smoking among those who were long-time cigarette quitters, women, younger, less educated, unemployed or retired, and non-users of alcohol.
HTPs could serve as a disincentive to successful quitting.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
HTPs should not be recommended as a cessation aid.
Educational interventions, in combination with intensified implementation of evidence-based tobacco control measures, are essential to eliminate the misperception that HTPs can be used as a smoking cessation aid and to denormalise the use of all types of tobacco, including HTPs.
Introduction
The increasing use of heated tobacco products (HTPs) has made tobacco control more challenging than ever before. The most common product, IQOS (Philip Morris International), has been approved by the US Food and Drug Administration for marketing as a ‘reduced exposure’ product on the grounds that the product has a lower level of specific harmful constituents than conventional cigarettes.1 2 Although this does not necessarily translate to a reduced risk of diseases,1 3 the tobacco industry has marketed HTPs as a ‘cleaner alternative to cigarettes’ and ‘reduced risk product’.4–6 Such claims may lead the public to perceive HTPs as a safe, effective aid for smoking cessation and undermine the public health efforts to denormalise the use of all types of tobacco.4 5 7
HTPs are already available in more than 40 countries, covering all regions of the world.8 Of those, Japan is the biggest market, where HTPs have established themselves as the second most used tobacco product.9 The increasing trend in HTP use has, however, levelled off in Japan in the recent few years. Following the first launch in 2014, the prevalence of current (past 30-day) HTP use skyrocketed 50-fold from 0.2% to 11.3% during 2015–2019,10 but remained at 10.9% in 2020 and 10.7% in 2021.11 12 In Japan, HTPs are regulated differently from conventional cigarettes or electronic cigarettes (e-cigarettes). The 2020 revised Health Promotion Act has placed more lenient restrictions on HTPs than those for conventional cigarettes, allowing people to use HTPs in designated rooms, while cigarette smoking is, in principle, prohibited in all indoor public places.13 E-cigarettes are not legally categorised as a tobacco product as they do not use tobacco leaf to generate aerosol. Furthermore, the sale of nicotine-containing e-liquids is banned under the Pharmaceutical Affairs Law,14 making Japan a fertile market for HTPs as the dominant novel tobacco product.9–11 15 16
In countries where HTPs were introduced earlier (eg, Japan, South Korea and several European countries), the products are now commonly used by cigarette smokers who attempt to quit smoking,17–19 despite there being no evidence to support the utility of HTPs as a cessation aid.3 Assessing the link between HTP use and smoking behaviours was a challenging task in the early phase of HTP use expansion due to short-term behavioural transitions of people who experimented HTPs (ie, ‘early adopters’). Kanai et al 20 recently studied 158 healthy male cigarette smokers in a Japanese workplace and found that concurrent users of HTPs were 23% less likely to quit tobacco than exclusive cigarette smokers. This was supported by a previous assessment conducted in Hong Kong that showed lack of association of HTP use with quitting smoking.21 Another prospective study suggests that, among former smokers, HTP use predicted smoking relapse at 1-year follow-up.16 There are also recent reports regarding the harms of HTPs, where HTP users experienced injurious acute effects on the cardiovascular system of similar magnitude to those of cigarette smokers.22 23 These findings enrich the evidence to negate the claim that HTPs are a safer alternative to help smokers quit.
To better understand the relationship between HTP use and smoking, however, there is a need for a larger-scale analysis that considers time-invariants and individual differences. Given that randomised controlled trials are not always realistic from an ethical standpoint, a longitudinal observation would be the most powerful and feasible design to detect prospective associations between HTP use and smoking behaviours in the naturalistic environment. With the 3 years since 2019 when the growth of HTP use reached a plateau, we are set to conduct the first longitudinal study to answer the important question: do HTPs help smokers quit? In the present study, we assessed two aspects of smoking behaviours, namely cessation and relapse, following HTP use during 2019–2021, using an internet-based survey of 7044 adults who were randomly derived from 2.3 million panellists.
Methods
Data
This study was a longitudinal analysis of the 2019, 2020 and 2021 waves from the Japan Society and New Tobacco Internet Survey (JASTIS), a nationwide, internet-based, self-reported survey of individuals aged 15 years or older in Japan. The initial JASTIS wave was administered in January–February 2015 using a private vendor, Rakuten Insight.24 Respondents were drawn from a pool of 2.3 million individuals by considering wide-ranging demographic and socioeconomic variables, including education, housing and marital status, as defined by the Japan census, and were asked to provide an online informed consent.15 From 2016 onwards, annual follow-up surveys have been conducted in/around February of each year with replenishment of the sample. Data collection was closed when the predetermined target sample size was met. More indepth details of the sampling methods for the JASTIS cohort have been described elsewhere.15 We obtained 9927 (2019), 9044 (2020) and 23 142 respondents (2021) in each wave after excluding individuals who provided irregular answers (9.7%–12.7% of all respondents in each wave) using a set of questions incorporated in the questionnaire.15 For example, individuals who checked all multiple-choice items of questions asking about illegal substance use (7 items) or presence of chronic conditions (15 items), those who answered with the same number over an entire set of questions, or those who chose a wrong answer to the question ‘Choose the second item from the bottom’ were excluded. In this study, we excluded individuals under the smoking age (20 years old) due to their volatility in tobacco use behaviours and a high dropout rate from the study. The analysis was restricted to adults aged 20–74 years who responded to all three waves during 2019–2021 (n=4476) and those who responded in 2 consecutive years (2019–2020 and 2020–2021, n=1734 and n=834, respectively; N=7044).
Exposure variable: current use of HTPs
The JASTIS assessed the use of all types of HTP that were available on the market at the time of data collection each year. Respondents were asked ‘How many days during the past 30-days did you use the following products?’ (answered with numbers 0–30) and were provided a list of product names and separate answer spaces for each product. We defined current HTP users as respondents who reported the use of any (one or more) HTP devices on ≥1 day in the past 30 days.
Outcome variables: smoking cessation and relapse
Respondents were asked whether they had ever smoked cigarettes during their lifetime. Those who responded ‘yes’ to the question were further asked about the number of days during the past 30 days on which they smoked cigarettes (answered with numbers 0–30). We categorised respondents into current (smoked on ≥1 day in the past 30 days), former (ever smoked during lifetime but did not smoke in the past 30 days) and never smokers. We assessed ≥1 month cessation as a change in smoking status from a current smoker at baseline to a former smoker at 1-year follow-up. Among those who observed ≥1 month cessation, we further determined cessation that had lasted for 6 months or longer as an indicator of successful cessation by asking respondents which stages they were at towards smoking cessation (‘How much are you interested in quitting smoking?’).25 The response categories included ‘I am not interested in quitting smoking’, ‘I am interested in quitting smoking some time’, ‘I intend to quit smoking within six months/one month’ and ‘I have already stopped smoking for less than six months/six months or longer’. The answer ‘I have already stopped smoking for six months or longer’ was defined as ≥6 months cessation.
Smoking relapse was assessed as a change in smoking status from a former smoker at baseline to a current smoker at 1-year follow-up.
Independent variables
On selection of independent variables, we identified known covariates of smoking and smoking cessation/relapse based on the literature.9 11 16 26–28 We then fitted multivariable exploratory models to identify and exclude factors that were highly correlated with other variables (variance inflation factors >10; see also the Statistical analysis section). Independent variables assessed in this study included the baseline survey year (2019, 2020), gender (male, female), age (20–29, 30–39, 40–49, 50–59, 60–74), education (high school or less, junior/some college, college (4 years) or higher), employment status (full time, part time, self-employed, unemployed/retired), self-rated health status (excellent/very good/good, fair/poor) and alcohol drinking (never/non-current, current (past 30 days)).
Among current smokers, the average number of cigarettes smoked per day was assessed (‘On average, how many cigarettes do (did) you smoke a day on the days you smoke(d)?’) as a proxy for smoking dependence.29 Respondents provided a numeric answer and were classified into three categories (1–9, 10–19 or 20+ cigarettes per day). Respondents were categorised as interested in quitting cigarette smoking if they answered ‘I am interested in quitting smoking some time’ or ‘I intend to quit smoking within six months/one month’ (vs ‘I am not interested in quitting smoking’) to the question ‘How much are you interested in quitting smoking?’ Past-year utilisation of evidence-based smoking cessation measures such as counselling services by healthcare professionals, prescribed medications and/or over-the-counter nicotine replacement therapy (NRT) products such as nicotine patches or gums was assessed (no/yes) as a proxy for previous quit attempts.
Among former smokers, respondents were asked about past-year smoking (‘Did you smoke in the past year?’) and were classified into two categories (smoked last time >1 year ago or within a year).
Statistical analysis
Using the discrete-time design, we treated respondents of each wave as an analytical unit to account for correlations within the same individuals who were included in both the 2019 and 2020 baseline cohorts. We fitted generalised estimating equation (GEE) Poisson models to compute adjusted prevalence ratios (APRs) of smoking cessation and relapse controlling for all the covariates listed (see the Independent variables section). To account for differences in demographic and behavioural characteristics of HTP users and non-users, multivariable analyses were weighted using the inverse probability weighting method.30 Propensity scores for ‘being an HTP user’ were calculated by fitting logistic regression models separately for current and former cigarette smokers adjusted for all the independent variables listed in the previous section. We calculated standardised difference as the difference in proportions between the exposed (HTP users) and non-exposed (HTP non-users) divided by the SD in the exposed group. We did not observe any imbalance that would potentially affect the validity of the analysis (ie, standardised differences <0.1 for all population subgroups).31 Unweighted analyses were also performed to confirm the reproducibility of the results. The 95% CIs were calculated using the robust variance estimator, also known as ‘sandwich’ variance estimator, assuming an unstructured correlation matrix within the same individual.32 Thirteen individuals were excluded from the multivariable analyses due to unknown educational attainment (provided an unclassifiable answer under the ‘other’ category). There were no missing values for all other assessed characteristics as they were required to be answered. For cessation outcomes, the analyses were restricted to current cigarette smokers who reported an established smoking habit. Using two separate questions, individuals who reported ‘I have smoked 100 or more cigarettes in total, or for six months or longer during lifetime’ and/or ‘I smoke/have smoked cigarettes regularly’ were defined as established smokers. Sixty-seven individuals were identified as non-established smokers and were excluded from the analyses, resulting in 1910 current established smokers being included. For smoking relapse, the analysis was restricted to former smokers (n=2906). To investigate the effect of current HTP use on smoking outcomes, we fitted separate GEE models within each of the assessed population subgroups using HTP non-users as the referent. Probability values for statistical tests were two-tailed, and p<0.05 was considered statistically significant. All analyses were performed using R V.4.0.3.
Results
Table 1 presents the baseline demographic characteristics and prevalence of current (past 30-day) cigarette smoking, HTP use and dual use (concurrent use of cigarettes and HTPs) in the 2019 and 2020 discrete-time cohorts combined. Overall, 17.2%, 9.1% and 6.1% reported current smoking, HTP use and dual use, respectively. 35.4% of current smokers reported concurrent use of HTPs, and 67.0% of current HTP users reported concurrent cigarette smoking. Among 1044 current HTP users, majority (n=739, 70.8%) used HTPs more than occasionally (ie, ≥5 days during the past 30 days) and 440 individuals (42.1%) were daily (all 30 days) users; 618 (59.2%) individuals reported having used ≥100 heated tobacco sticks within the past 30 days (data not presented). Smoking status and HTP use across survey years are shown in online supplemental table 1. Unweighted and weighted demographic distributions of current and former smokers are presented in online supplemental table 2.
Supplemental material
Supplemental material
Baseline characteristics of the respondents: 2019 and 2020 discrete-time cohorts and prevalence of current cigarette smoking, HTP use and dual use, JASTIS study, Japan
Table 2 presents the APRs for the associated factors of smoking cessation. Established smokers who reported smoking 10–19 cigarettes and 20+ cigarettes per day had lower likelihood of ≥1 month cessation (APR=0.67 (95% CI 0.54 to 0.83) and 0.58 (95% CI 0.44 to 0.76), respectively) compared with those reported smoking 1–9 cigarettes per day. Another characteristic that was negatively associated with ≥1 month cessation was being self-employed (APR=0.63 (95% CI 0.41 to 0.97)) versus working full time. Notably, the likelihood of ≥1 month cessation was 1.65 (95% CI 1.37 to 2.00) times higher during 2020–2021 than during 2019–2020. A higher likelihood of ≥1 month cessation was also seen among smokers who were interested in quitting smoking (APR=1.36 (95% CI 1.09 to 1.69)) than those who were not, those with junior/some college education (APR=1.36 (95% CI 1.03 to 1.80) vs high school or less) and those unemployed/retired (APR=1.30 (95% CI 1.01 to 1.69) vs working full time). Although there was a similar pattern for ≥6 months cessation, education and employment status did not show significant associations. Older age (60–74 years) was positively associated with ≥6 months cessation (APR=1.65 (95% CI 1.01 to 2.67)), while this did not show significant association with ≥1 month cessation.
APR for factors associated with smoking cessation among established cigarette smokers, inverse probability weighting, 2019–2021, JASTIS study, Japan
Figure 1 presents the associations between HTP use and smoking cessation within each population subgroup. Among established cigarette smokers who had used evidence-based cessation measures such as counselling services, prescribed medications and/or over-the-counter NRT products, current users of HTPs had a lower likelihood of ≥1 month cessation (APR=0.61 (95% CI 0.39 to 0.95)) compared with those who did not use such measures. Among smokers who reported smoking 20+ cigarettes per day, concurrent use of HTP was significantly associated with a decreased likelihood of ≥1 month cessation (APR=0.62 (95% CI 0.39 to 0.99)) compared with HTP non-users. Similarly, HTP use was negatively associated with ≥1 month cessation among those who reported high school education or less (APR=0.73 (95% CI 0.54 to 0.97)) and fair/poor health status (APR=0.59 (95% CI 0.35 to 0.99)). For ≥6 months cessation, negative associations with HTP use were seen among those aged 20–29 years (APR=0.56 (95% CI 0.28 to 0.99)) and among full-time workers (APR=0.56 (95% CI 0.38 to 0.83)).

Associations between HTP use and indicators of smoking cessation among established cigarette smokers, inverse probability weighting, 2019–2021, JASTIS study, Japan. Current cigarette smoking was defined as smoking cigarettes including roll-your-own cigarettes in the past 30 days. Established smokers were current (past 30-day) smokers who reported having smoked ≥100 cigarettes, smoked for ≥6 months and/or smoked regularly during their lifetime (n=1910). Respondents of each wave were treated as an analytical unit using the discrete-time design. Data were weighted using the inverse probability weighting method to account for differences in the demographic and behavioural characteristics of HTP users and non-users. APRs were computed using separate generalised estimating equation Poisson models for each of the assessed population subgroups. 95% CIs were calculated using the robust variance estimator. The models were adjusted for all variables listed in the figure. Bold values represent statistically significant results (p<0.05). 1≥1 month smoking cessation was defined as a change in cigarette smoking status from current (past 30-day) smoker at baseline to former smoker at 1-year follow-up. ≥6 months cessation was identified using the report ‘I have already stopped smoking for ≥6 months’ at the time of data collection. 2Utilisation of counselling services by healthcare professionals, prescribed medications and/or over-the-counter nicotine replacement products (nicotine patches, gums, etc) in the past year. APR, adjusted prevalence ratio; HTP, heated tobacco product; JASTIS, Japan Society and New Tobacco Internet Survey; ref, referent.
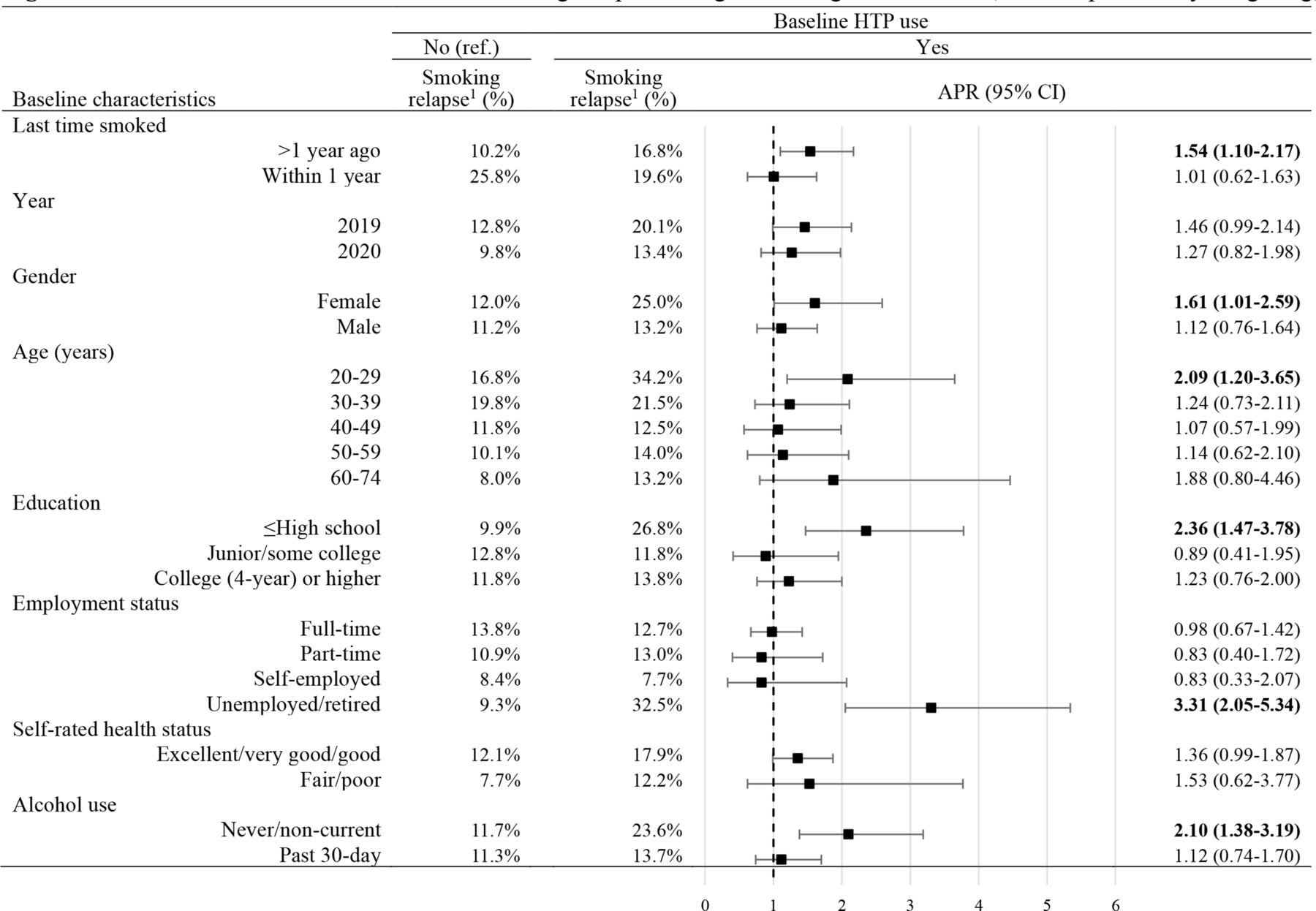
Table 3 presents the APRs for the associated factors of smoking relapse. Among former cigarette smokers, current HTP users were 1.39 (95% CI 1.02 to 1.89) times more likely to relapse to smoking at 1-year follow-up compared with those who did not use HTP. Those who last smoked within a year had 1.62 (95% CI 1.17 to 2.25) times higher likelihood of relapse compared with those who last smoked >1 year ago. By contrast, lower likelihoods of relapse were observed during 2020–2021 (APR=0.74 (95% CI 0.56 to 0.99)) versus 2019–2020, and among individuals aged 40–49 years (APR=0.59 (95% CI 0.37 to 0.96)), 50–59 years (APR=0.55 (95% CI 0.32 to 0.94)) and 60–74 years (APR=0.42 (95% CI 0.23 to 0.78)) versus 20–29 years. Stratified analyses showed that former smokers who last smoked >1 year ago and currently used HTPs had 1.54 (95% CI 1.10 to 2.17) times higher likelihood of smoking relapse than HTP non-users (figure 2). Significant positive associations between HTP use and smoking relapse were also observed among female former smokers (APR=1.61 (95% CI 1.01 to 2.59)), thosed aged 20-29 years (APR=2.09 (95% CI 1.20 to 3.65)), those with high school education or less (APR=2.36 (95% CI 1.47 to 3.78)), those who were unemployed/retired (APR=3.31 (95% CI 2.05 to 5.34)) and never/non-current users of alcohol (APR=2.10 (95% CI 1.38 to 3.19)).

{kind=link}
{kind=link}
Associations between HTP use and smoking relapse among former cigarette smokers, inverse probability weighting, 2019–2021, JASTIS study, Japan. Former smokers were those who smoked during their lifetime but not in the past 30 days (n=2906). Respondents of each wave were treated as an analytical unit using the discrete-time design. Data were weighted using the inverse probability weighting method to account for differences in the demographic and behavioural characteristics of HTP users and non-users. APRs were computed using separate generalised estimating equation Poisson models for each of the assessed population subgroups. 95% CIs were calculated using the robust variance estimator. The models were adjusted for all variables listed in the figure. Bold values represent statistically significant results (p<0.05). 1Smoking relapse was defined as a change in cigarette smoking status from former smoker at baseline to current (past 30-day) smoker at 1-year follow-up. APR, adjusted prevalence ratio; HTP, heated tobacco product; JASTIS, Japan Society and New Tobacco Internet Survey; ref, referent.
APR for factors associated with smoking relapse among former cigarette smokers, inverse probability weighting, 2019–2021, JASTIS study, Japan
Consistent results were obtained from the unweighted analyses and are presented in online supplemental tables 3–6.
Supplemental material
Supplemental material
Supplemental material
Supplemental material
Discussion
HTP use did not help smokers quit or prevent former smokers from relapsing. HTP use was significantly associated with a lower likelihood of ≥1 month cessation among established cigarette smokers who had used evidence-based cessation measures such as counselling services by healthcare professionals, prescribed medications and/or over-the-counter NRT products in the past year, and those who reported smoking 20+ cigarettes a day, high school education or less, and fair/poor health status. HTP use was also linked to a decreased likelihood of longer-term (≥6 months) cessation among established smokers aged 20–29 years and full-time workers. These findings negate the widespread misperception that HTPs can be used as a smoking cessation aid. Furthermore, HTP use was significantly associated with smoking relapse among former cigarette smokers overall and within some subgroups, including those who had stopped smoking for >1 year, women, those with high school education or less, those who were unemployed or retired, and never or non-current alcohol users. Interventions are needed to educate the public not to rely on HTPs for quitting smoking and to encourage use of evidence-based cessation resources.
In the present study, none of the assessed subgroups of established smokers showed positive associations between HTP use and smoking cessation, indicating that HTPs could serve as a disincentive to successful quitting and not as a cessation aid. This is unsurprising given that dual users of HTPs and cigarettes are equally dependent on tobacco compared with exclusive cigarette smokers.33 Our findings were aligned with those from a study of healthy Japanese male workers showing that dual users of HTPs and cigarettes were less likely to quit tobacco relative to exclusive cigarette smokers.20 Stratified analyses in the present study revealed that such negative associations were not limited to male workers, but were also found in other populations. We also confirmed the link between HTP use and elevated risk of smoking relapse among former smokers. HTP use did not reduce smoking relapse in any of the population subgroups assessed, negating the claim for HTPs as an alternative to cigarettes towards cessation efforts. In particular, we observed that those who had stopped smoking for a long time (>1 year) were more likely to relapse to smoking when they used HTPs. Considering that tobacco dependence is likely maintained even if smokers have switched from cigarettes to HTPs,16 33 further longitudinal research is needed to elucidate the pathway of smoking, switching, cessation and relapse.
It is notable that, when we compared the changes in smoking behaviours between the two baseline years, namely 2019 and 2020, the latter showed a significantly greater likelihood of smoking cessation and a lower likelihood of relapse. This is likely due to the combined effects of social, environmental and individual changes that occurred during 2020–2021. Such changes may include lifestyle changes due to stay-at-home recommendations under the COVID-19 pandemic, increased awareness that smoking is one of the risk factors for severe illness and mortality from COVID-19,34 tobacco tax increase in October 2020,35 and enactment of the revised Health Promotion Act which bans indoor public smoking.13 As these changes are expected to be maintained and orient long-term behavioural patterns in the ‘new normal’ life, it is essential to monitor their effects and magnitude on smoking behaviours, which might vary across populations.
Parties to the WHO Framework Convention on Tobacco Control, including Japan, are responsible for implementing MPOWER, a set of six evidence-based tobacco control measures.7 The global increase in HTP use has posed challenges to all components of MPOWER.5 7 Monitoring tobacco use (M in MPOWER) has become more complex than ever before due to misperceptions of HTP users that they do not think of themselves as a tobacco user or confuse HTPs with e-cigarettes.26 Timely enactment of laws is required to protect the public from exposure to secondhand HTP emissions (P in MPOWER), mandate warning labels on HTP devices (W in MPOWER), enforce bans on HTP promotions that may evoke curiosity to tobacco use (E in MPOWER) and raise the excise tax rate on HTPs to the same level as that for conventional tobacco (R in MPOWER). Our findings, in particular, suggest that HTPs could undermine the efforts to offer help to quit smoking (O in MPOWER); among established smokers who had used evidence-based cessation measures, ≥1 month cessation was less likely observed when they used HTPs (APR=0.66 vs non-users). The misperception that HTPs help smokers quit is widespread. A recent study of 28 European countries revealed that nearly one-third of current HTP users reported using the product for stopping or reducing cigarette smoking.17 In Japan, HTP is the most common measure to give up smoking, with over 50% of smokers who attempted to quit reporting using it, while only 15% reported attending a cessation clinic.18 Indeed, the number of patients who used cessation clinics in Japan has sharply declined by 68% during 2014–202036 following the introduction of HTPs to the market. While this may be due to a lack of impactful interventions to motivate smokers to quit (eg, price increase), we cannot rule out the possibility that increased use of HTPs led smokers away from evidence-based cessation services. Similarly, a decline in clinic visits for smoking cessation was observed in South Korea after HTPs were put on the market in 2017.37 Educational interventions, in combination with intensified implementation of MPOWER, are essential to eliminate the misperception that HTPs help smokers quit and to increase utilisation of evidence-based cessation resources. Considering together with recent reports on the deleterious health effects of HTPs,22 23 healthcare providers should understand and advise patients that HTPs are not free from harm and can make quitting even more difficult.
This study is subject to several limitations. First, the definition of exposure in this study considered respondents’ HTP use only during the 30 days before data collection and did not consider short-term HTP use that may have occurred out of this period or occasional (less than monthly) HTP use. However, we reduced such potentially unmeasured exposure as much as possible by using the most recent data from the 2019–2021 surveys. Given that HTP use in Japan has passed the initial phase of expansion and has reached a plateau since 2019,10 11 38 we assume that our sample did not include many experimenters or ‘early adopters’, who would initiate and stop using HTPs in a short period. The exposure measure in our study can be interpreted as a proxy for regular HTP use, as the majority of past 30-day HTP users were, even by a conservative definition, established users (having used ≥100 heated tobacco sticks in the past month). Continuing longitudinal observation is essential to understand the trajectories of HTP use and smoking and to establish causal relationships. It will also be of importance to investigate detailed HTP use patterns, including the amount used and the type of product. Second, both the exposure and outcome variables were self-reported, which might have resulted in misrecall or social desirability bias; however, self-report on tobacco use status was previously validated.39 Third, as the survey was internet-based and the analyses were restricted to individuals who completed at least two survey waves, our sample might not represent the Japanese population. However, over 90% of the population has access to the internet as of 2021,40 and smoking prevalence in our study sample (17.2%) was similar to that of the nationally representative adult cohort (16.7%).41 Furthermore, as we conducted multivariable-adjusted analyses for the subset populations of former and current smokers, this limitation does not affect the implications of our findings. Fourth, the results from the multivariable analyses should be interpreted with caution as tobacco use behaviours might have been affected by unmeasured ecological or individual factors. Lastly, our findings might not be generalisable to other countries due to the different availability of tobacco products and regulations. Further evidence is needed for a more comprehensive understanding of the interaction between HTP use and smoking in different societies.
Conclusion
HTP use did not help cigarette smokers quit or prevent former smokers from relapsing. Educational interventions, in combination with intensified implementation of evidence-based tobacco control measures, are essential to eliminate the misperception that HTPs can be used as a smoking cessation aid and to denormalise the use of all types of tobacco, including HTPs.
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the author (TT) upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by the Research Ethics Committee of the Osaka International Cancer Institute (no: 20094-2). Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SO and KT equally contributed to designing the study. SO conducted data analysis and drafted the manuscript. TT designed the survey, monitored data collection, and conceptualised the study. TT is responsible for the overall content as guarantor. All authors contributed to data interpretation and critically reviewed and revised the manuscript.
Funding This study was supported by the Japan Society for the Promotion of Science KAKENHI Grant (#21H04856) and Health Labour Sciences Research Grant (#19FA1005, 19FA1012, 19FA1011 and 20FA1005).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.